
Comprehensive physiology testing of both the epicardial arteries and microcirculation, with new technologies available through partnership with your interventional cardiologist, can provide a clear assessment of Coronary Microvascular Dysfunction (CMD) to help guide treatment and outcomes.2 As CMD is no longer a diagnosis of exclusion, a clear diagnosis of CMD can help patients take the first step to improve their Quality of Life (QoL).3

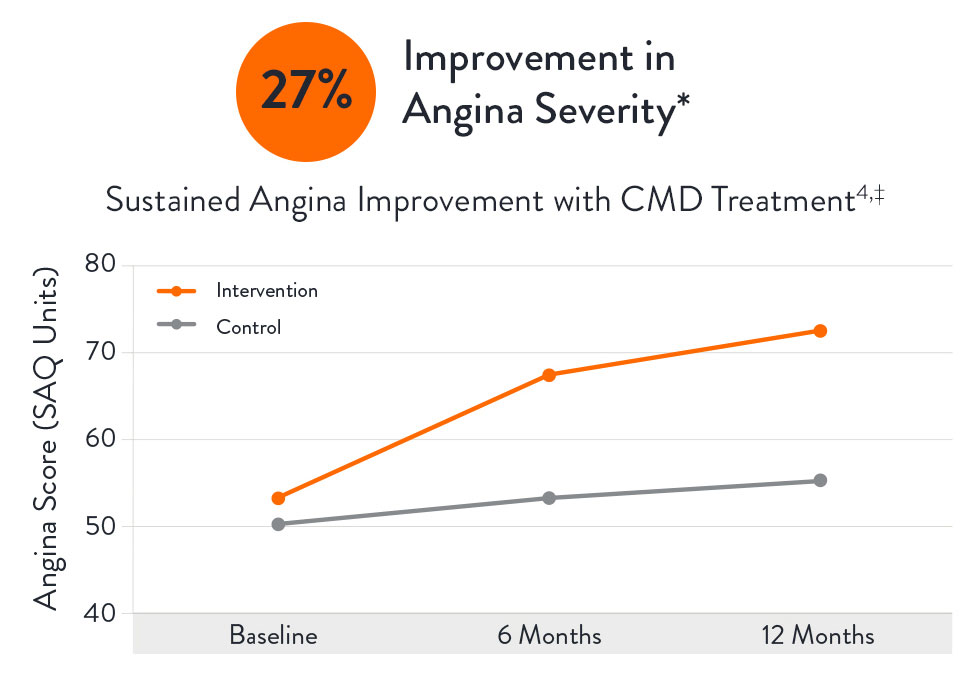
The CorMicA (CORonary MICrovascular Angina) study revealed that patients may benefit when CMD is accurately diagnosed and appropriately treated, with patients showing a 27% improvement in angina severity following diagnosis at 12 months.3
An accurate CMD diagnosis can help reduce healthcare resource consumption,2 resulting in lower costs for hospitals and patients4 with a savings from $2,100 (Netherlands) to $7,300 (U.S.) per hospitalization avoided (2017 costs).5 Additionally, an economic analysis of the CorMicA study showed that a comprehensive physiology assessment is cost-effective compared to standard care (medical therapy and cardiac rehabilitation care) at 1-year follow-up.6
Connect with your interventional cardiologist to determine how the PressureWire™ X Guidewire and CoroFlow‡ Cardiovascular System can benefit your patients with no angiographic abnormalities.
Learn more about PressureWire™ X Guidewire and CoroFlow‡ Cardiovascular System.

European and American guidelines provide a class 2a recommendation for a physiology wire-based assessment for patients with stable chest pain and/Ischemia and No Obstructive Coronary Artery Disease (INOCA).8,9
The ESC guidelines8 2019 were updated accordingly to include an increased focus on microvascular dysfunction.

The AHA/ACC Clinical Practice Guideline9 on chest pain includes Class IIa recommendation for guidewire-based assessment for ischemia and no obstructed coronary artery disease (INOCA) patients.

CFR = coronary flow reserve; CMR = cardiac magnetic resonance; ECG = electrocardiogram;
FFR = fractional flow reserve; iwFR = instantaneous wave-free ratio; LAD = left anterior descending; PET = position emission tomography.
a Class of recommendation
b Level of evidence
Level-NR: Level (Quality) of Evidence Level B-NR (non-randomized): moderate-quality evidence from 1 or more well-designed, well-executed non-randomized studies, observational studies or registry studies. RCTs. Meta-analyses of such studies.
*With Index of Microcirculatory Resistance (IMR), Coronary Flow Reserve (CFR), Fractional Flow Reserve (FFR) and Resting Full-Cycle Ratio (RFR).
MAT-2207041 v2.0
You are about to enter an Abbott country- or region-specific website.
Please be aware that the website you have requested is intended for the residents of a particular country or countries, as noted on that site. As a result, the site may contain information on pharmaceuticals, medical devices and other products or uses of those products that are not approved in other countries or regions
Do you wish to continue and enter this website?
MAT-2305078 v1.0