
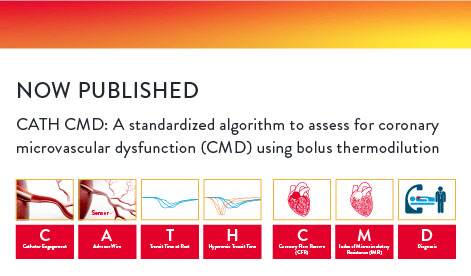
CATH CMD is a global algorithm that captures the essential details of performing the bolus thermodilution workflow and assists in decision-making in a simple and stepwise manner. In summary, CATH captures the how to perform bolus thermodilution and CMD captures the what to do with the Index of Microcirculatory Resistance (IMR) and Coronary Flow Reserve (CFR) measurements to provide a diagnosis of Coronary Microvascular Dysfunction (CMD).
A full physiology assessment (with Resting full-cycle Ratio (RFR), Fractional Flow Reserve (FFR), IMR and CFR) of the epicardial arteries and the microvasculature can provide patients with persistent angina an accurate diagnosis to improve outcomes.1
Did you know a standardized approach to CMD assessment can enhance your workflow in the cath lab? Learn how the CATH CMD algorithm can help streamline the assessment of CMD and improve patient outcomes.



*Repeat measurement of Tmnrest

*Decrease in pressure, patient symptoms, FFR drop
**Repeat measurement of Tmnhyp

*Evolving concensus


*Evolving consensus

GTN (glyceryl trinitrate) | NTG (nitroglycerin) | LAD (left anterior descending) | FFR (fractional flow reserve) | IMRcorr (IMR corrected) | CMD (coronary microvascular dysfunction) | Tmnrest (resting transit mean time) | Tmnhyp (hyperemic transit mean time)
Dr. Tom Ford
Prof. Filippo Crea, MD
An Interview with Dr. Takayuki Warisawa
An Interview with Dr. Tommaso Gori
An Interview with Dr. William Fearon
An Interview with Dr. Andy Yong

Dr. Tom Ford

Prof. Filippo Crea, MD

An Interview with Dr. Takayuki Warisawa

An Interview with Dr. Tommaso Gori

An Interview with Dr. William Fearon

An Interview with Dr. Andy Yong
MAT-2211746 v3.0
You are about to enter an Abbott country- or region-specific website.
Please be aware that the website you have requested is intended for the residents of a particular country or countries, as noted on that site. As a result, the site may contain information on pharmaceuticals, medical devices and other products or uses of those products that are not approved in other countries or regions
Do you wish to continue and enter this website?
MAT-2305078 v1.0